© 2012 M. Nafte
2012 – № 2 (4)
Key words: syphilis, sexually transmitted infections, HIV/AIDs, public health, syndemics, MSM, contagion, stigma
Abstract: In the paper, the author examines what has been described as an epidemic of venereal syphilis in the city of Toronto, Canada from the year 2000 to 2010, as a means of ascertaining whether syphilis is indeed increasing, and if it is interacting syndemically with other infectious ailments, specifically HIV/AIDs. The author presumes, that syphilis might have only been eradicated from the collective memory, and has been busy steadily adapting to various populations for the last five centuries.
Introduction
Sexually transmitted infections (STIs) have been a constant presence in human populations for many centuries. Syphilis–Treponema pallidum–in particular has a rich place in history as one of the most virulent and deadly, and culturally transforming. From Konrad Schelling’s earliest descriptions of the pustulis malas morbum –‘disease of bad pustules’– in the late 1400s (Holcomb, 1938), Fournier’s 19th century comprehensive overview of hereditary syphilis (Howles, 1943), to Schaudinn and Hoffman’s 20th century discovery of the Spirochetea pallida, this infectious disease has been the subject of intense interest and debate for over 500 years, reflecting a curious mix of shame, romanticism and power that still resonates today.
As a re-emerging infectious disease in the Western world, syphilis is once again the center of public health campaigns aimed at screening, controlling and reducing its increased occurrence, specifically in “MSM communities” (men who have sex with men). In this paper, I examine what has been described as an epidemic of venereal syphilis in the city of Toronto, Canada from the year 2000 to 2010, as a means of ascertaining whether syphilis is indeed increasing, and if it is interacting syndemically with other infectious ailments, specifically HIV/AIDs as implied by Singer and Clair (2003). In turn, I compare the purported rates of syphilis among MSM with the numbers attributed to immigrant and refugee populations in Canada, in order to question the appropriateness of the term “outbreak” and “community” as applied to MSM in Toronto, as well as to resituate the context in which syphilis may be occurring in the broader population.
Underscoring this analysis are questions around whether the treatment and cure of syphilis have at all been successful over the last several decades, and if an “epidemic” of syphilis can be better understood as a cluster of syphilis testing among MSM, compared with a virtual absence of routine testing in the broader population. Though the reduction in rates of this infectious disease has been attributed to the development of antibiotics in the 20th century (Baughn and Musher, 2005), it has been proposed that antibiotics are actually ineffective and only serve to suppress the symptoms but not the disease itself (Margulis et al, 2009). This dramatic departure from what is considered a firmly established medical position suggests that syphilis might have only been eradicated from our collective memory, and has been busy steadily adapting to various populations for the last five centuries. This perspective is discussed further in light of the current worldwide syphilis increase, and its intimate relationship with AIDS and HIV.
A Brief History of Syphilization
In Fracastoro’s 16th century poem, he named the dreaded blight “Syphilis” after a fictitious shepherd (Sifilo) who had dared to defy the sun god Apollo and was struck down by sores. According to the Italian physician-astronomer-poet (1478–1553), syphilis was thought to have come about by noxious air yet Fracastoro warned his readers to “abstain however from the act of love” else “blotches over the body spread, profane the bosom and deform the head” (Fracastoro, 1930, p.741). As a prestigious court physician who began to see an outbreak among his exclusive patients, he distinguished it clearly as an “epidemic distemper; a perpetual grief” that would last so long that everyone would forget its clinical description and name (Fracastoro, 1930, p.740). By this means, Fracastoro defined the “temporal and spatial limits” (Herring and Swedlund, 2010, p.9) of this new scourge based on the fact that rulers, popes, noblemen, clerics and bishops across a prospering Europe were increasingly afflicted despite their wealth and status.
Though the slum-dwellers, prostitutes and the destitute were in fact well represented, they inevitably provided the bodies upon which the disease was explored and made visible1. In the 17th to 19th century era of the autopsy, the private collections and public displays of human specimens bearing advanced syphilitic lesions would teach, shock, repel and fascinate a paying audience (Bates, 2008; Richardson, 2001; Sappol, 2002). Public anatomy museums and the homes of certain independent physicians across Europe served as places for public health and anatomical education where gentlemen and unescorted ladies could view diseased genitalia and access discreet treatments for their “perpetual grief” often more deadly than the disease (Bates, 2008).
That infectious disease is very much a “social entity and thus socially constructed” (Rosenberg, 2003, p. 498), as well as a “prime mover in cultural transformation” (Inhorn and Brown, 1990, p. 89) is nowhere more historically evident than with the emergence of syphilis across Europe and eventually, North America. The medical literature and the later century pamphlets, posters and brochures were replete with images of the grotesque, the miserable and the suffering. They all described “the evil pox”2 as one that brought on madness, deformity and an agonizing death. Art, medicine, politics, literature, and music were informed by the syphilitic face, head and body, or the descent into madness brought about by its later stages (see Gilman, 1995; Greenspan, 2006; Sherman, 2006). It set healthy bodies apart from diseased bodies, defined national borders, created a new vocabulary of affliction, and entered the European consciousness as a disease of the degenerate that contaminated the learned, and the nobility.
As the virulence and morbidity of syphilis slowly decreased from the 16th to the 19th century, Europe’s intellectuals defined its ubiquitous presence as one that was a natural consequence of careless aristocrats, the spirit of adventure, and male rakishness. The dreaded pox was often considered inevitable for young men on war campaigns, vacation and world travel, and many references to it were humorous and facetious (Moore, 1939). Shakespeare’s work often references the “pox” as the upshot of misguided love, and the introduction to Rabelais’s (1494–1593) first novel Gargantua is dedicated to “you thrice precious pockified blades”. Catholic priest and humanist Erasmus (1436–1536) maintained that to have syphilis was to be ignobilis et rusticans –‘of noble birth and the peasantry’ (Cartwright, 1972; Moore, 1939).
According to Fabricius (1994) syphilis not only contributed to an understanding of human despair and suffering, it shaped the early modern period of medicine in its approach to professionalism and a scientific method. While the disease was imbued with metaphors of wanton sexuality and degeneracy it also provided a growing body of doctors and scientists the opportunity to examine the mysterious ‘seeds of contagion’ (Fracastoro, 1930) that caused various afflictions.
Aside from periodic outbreaks across Europe and North America, syphilis entered the early 20th century as a disease to observe, manipulate and control, once again in the bodies of the destitute and the poor. The 19th and early 20th century era of public health service research on syphilis is exemplified by the Oslo study of 1890 to 1910 (Clark and Danbolt, 1955), the infamous Tuskegee experiments from 1932 to 1972 (Jones, 1993), and the less well known Guatemalan prisoner experiments from 1946 to 19483. Like many of the mishaps with mercury and arsenic from centuries prior, physicians with unrestricted access to the bodies of the marginalized tested out the effectiveness of promising new cures, or ventured to observe the untreated progression of the infection in all of its stages, rationalized as a campaign for the greater good.
With the arrival of penicillin-antibiotics after World War II syphilis became a curable ailment and its prevalence was drastically reduced in many countries (Baughn and Musher, 2005). Along with the other STIs in the Western world, such as gonorrhea, herpes, and later chlamydia, syphilis was considered to be yet another treatable disease and for the most part ignored (Baughn and Musher 2005; Golden et al. 2003). For many in the Western world with unlimited access to testing and treatment, STIs were merely part of “the hazards of a busy sexual lifestyle” (Gorman, 1986, p.163).
The sudden emergence of AIDS in North America in the late 1970s radically transformed the biocultural landscape. Untreated syphilis was suddenly deposed as the most fatal sexually transmitted infection by what was then viewed as an incurable viral scourge. By the 1990s syphilis was considered rare; a controlled infectious disease that no longer contributed to, nor transformed Western culture by way of art, literature, music or madness. Neither did it generate a plethora of research, bulletins or reports in the media as it once had. Its metaphoric force suddenly disappeared, displaced by another fatal sexual disease. In the era of AIDS, powerful new metaphors flourished (Sontag, 1988) while syphilis was “relegated to the pages of forgotten history” (Baughn and Musher, 2005, p.206). At that point in time, most young, Western doctors had never seen syphilis in its various manifestations or stages, and would not know how or when to test for it (Pao et al., 2002).
Given its overall rate of decline in the late 1990s, it is surprising that there has been a “sudden resurgence” of infectious syphilis worldwide with rates currently rising “more than tenfold” (Klausner et al., 2005). The trend has also been recorded in Canada and the United States, defined as “rapidly increasing” and as in other European countries, according to their public health reports, syphilis is predominantly affecting men who have sex with men (MSM) (Aadland et al., 2010; Wheater et al., 2003; Leber et al., 2008).
Syndemics and STIs
In the 1990s, Merrill Singer, as part of a network of critical medical anthropologists (see also Farmer, 1999; Saussy, 2010) formalized the concept of syndemics in his work on AIDS, substance abuse and violence within a Puerto Rican community in Hartford, Connecticut (Singer, 1996). In it he maintained that neither drug abuse, gang violence or AIDS could be understood as separate or simultaneous issues but each was better understood as a complex web of components that reinforced and were reinforcing one another4. Factors such as alcoholism, poverty, unemployment, low educational levels and gang violence were creating and contributing to the health crisis plaguing the Puerto Rican community, as well as most other contemporary inner cities in the United States. These were in turn strongly influenced by a broader array of political-economic and social factors.
In a more recent study among inner city African American and Puerto Rican heterosexuals, Singer et al. (2006) argue that high rates of STIs, namely gonorrhea, chlamydia and AIDS, are as a result of a “cultural logic” shaped by an inner city life of domestic violence, limited expectations of the future, impoverished family life, and a lack of positive role models. The use of this cultural logic, which entails very little to no relationship trust, a fear of attachment, and patterns of condom use and disuse, leads individuals to make poor choices, and thus experience a high level of risk. In short, according to Singer et al. (2006; 2019) it is “a rational response to social disparity”.
The inherent connection between sexually transmitted infections, cultural dynamics, and socioeconomic factors is underscored in a number of studies (Farmer, 1992; Singer, 1996; Farmer, 1999; Singer et al., 2006; Chesson et al., 2005; Operario and Nemoto, 2010; Stall et al., 2007; and Uretsky, 2010). These studies provide an alternative perspective for examining the incidence of STI clusters in particular populations. Rather than emphasizing irresponsibility, immorality, or poor values as factors contributing to sexually transmitted disease, such research introduces a more integrated evaluation. More importantly, it demonstrates better and effective strategies in combating STIs through sound, multilevel interventions.
Applying the syndemic framework to the cluster of venereal syphilis cases among MSM in the City of Toronto however, proves far more challenging. Are factors such as alcoholism, drug abuse, gang violence, and a broader array of socio-economic and political issues contributing to the sudden increase of the infectious disease among middle-aged urban males? An overview of the data and the literature reveals that there was not only a paucity of sources that could indicate such synergistic relationships but an overall disjuncture in what denotes a community, an epidemic and an outbreak.
Community: Identity vs. Behaviour
The city of Toronto has a population of approximately 2.49 million and 5.5 million if its suburbs are included. Half of this population is said to have been born outside of Canada, and more than half of all immigrants in the city of Toronto are aged 30 years and over (Toronto Data Fact Sheet, 2011). Toronto is said to be one of the most ethnically and culturally diverse cities in the world where over 140 languages and dialects are spoken, and over 200 distinct ethnic groups reside. How many of these individuals are “men having sex with men” is not noted in any of these fact sheets.
Nonetheless, Toronto is known for a thriving gay culture and in many of the city websites there is tourist type information designed to orient visitors, and introduce locals to the vibrant gay scene. Locations for “gay friendly” or “gay run” shops, bookstores, events and clubs are listed along with historical facts and links to other gay, or “queer” related resources.
Defining a gay, queer or MSM community can thus be quite simple when it comes to social media, events, clubs, parades, and literature. But when it comes to public health discourse, infectious disease reporting, statistics, treatment and screening, the actual boundaries of the community become more ambiguous, and its membership less understood.
Whether it is identity or behaviour that create and bind a community, both are seen to be inherently dynamic yet ambiguous notions. As Cornell and Hartmann (1998), and Trostle (2005) assert, groups of people sharing common cultural categories are active agents in the making and remaking of their own identities. These identities and categories change over time as the boundaries separating members from nonmembers are renegotiated, and membership is constantly redefined. The construction of identity is therefore not a one time act but continuous and historical. Moreover, one community may be geographically and ethnically distinct, and perceived as being more authentic, while another may be based only on shared interests and sustainability. We may think we recognize a distinct community by certain and more tangible attributes, but these are also often largely symbolic with constructed narratives of unity and belonging, despite a variety of experiences, identities and differences (see McDonald, 2006; Cornell and Hartmann, 1998).
The moniker “MSM” used to define a community that encompasses a specifically gay community, distorts rather than distinguishes its parameters. Men who have sex with men are not necessarily “gay” or living in the designated gay friendly parts of the city. Many may be bisexual, married to women, transgendered, or neither of these. The term MSM is taken to be a neutral term that reflects sporadic or long-term behaviour, rather than identity, whereas the term ‘gay’ denotes a cultural identity, not behavior5. To overlap these concepts to make one ambiguous community entails a loss of authenticity. Furthermore, according to Young and Meyer (2004, pp. 1144-1149) “to label as MSM and WSW (women who have sex with women) people who describe themselves as gay or lesbian, or use another identity term is to deny their self-labeling and, by extension, their self-determination”. Hence, the term not only creates ambiguity, it has also become stigmatizing.
As such, the issues around self-labeling, the use of language to mediate stigma, concepts of community, and behaviour versus identity, can confound more than clarify the boundaries of disease contagion. In the midst of an ‘epidemic’, whether it is HIV or syphilis, these embedded issues come to reveal less about the course of an infectious disease and indeed more about the relationship between “ideology, social structure and the construction of particular selves” as Rosenberg (1992, p.279) maintains.
Sex in the City? Syphilis and Toronto
According to the data available on Toronto Public Health websites, the Canadian Institute of Health Research, as well as Reynolds et al. (1998), Leber et al. (2008) and Mishra et al. (2011), the incidence of reported syphilis is increasing in the city of Toronto; 95 percent among men who have sex with men. It is interacting and manifesting rapidly with other infectious diseases, specifically HIV (see Figures 1 and 2). Between 1997 and 2006 infectious syphilis rates increased by 1,050 percent (Canadian Institute of Health Research, 2008). For 2008, the largest number of cases in Toronto was seen in males aged 40 to 44 years (Figure 3) and the largest increase is recorded in males aged 15 to 34 years, as it is for HIV rates.
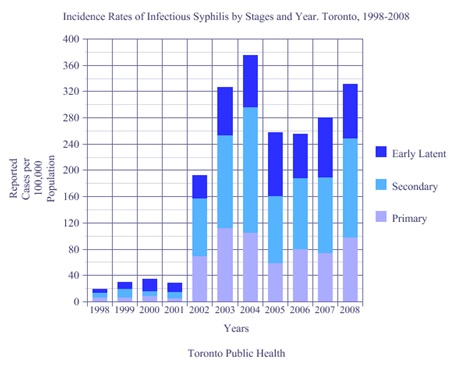
Figure1. Incidence Rates of Infectious Syphilis. Data from Toronto Public Health (2008)
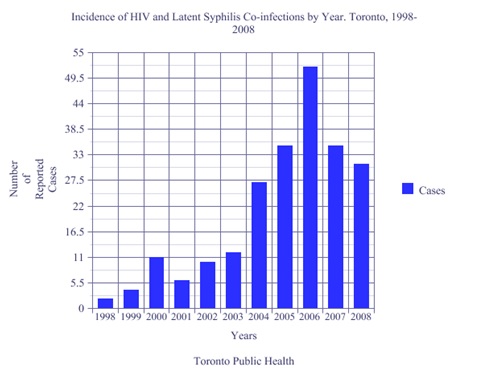
Figure 2. Incidence of HIV and Latent Syphilis Co-infection. Data from Toronto Public Health (2008)
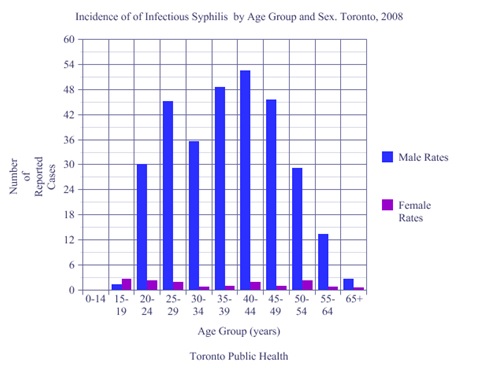
Figure 3. Incidence of Infectious Syphilis. Data from Toronto Public Health (2008)
HIV infected males (61 percent of those tested positive for syphilis) are said to be contracting syphilis primarily through unprotected oral sex, which was considered “safe” in the prevention of HIV but high risk for syphilis (Wheater et al., 2005; Wong et al., 2005; Zetola and Klausner, 2006). They are also contracting HIV when unknowingly infected with syphilis through primary lesions that are larger and deeper, facilitating both the transmission of the virus and the acquisition of HIV infection (Fenton et al., 2008; Chesson et al., 2005; Zetola and Klausner, 2007; Karp, 2009). With HIV coinfection, syphilis increases in virulence, and progresses rapidly and aggressively through its stages. What would normally take years to advance through primary, secondary and tertiary stages of syphilis, takes months in an HIV infected person (Karp, 2009; Nnonuka and Ezeoke, 2005; Miller and Hicks, 2010).
Leber et al. (2008) stress that the syphilis epidemic is increasing because it is being reintroduced to an “MSM population” by an already infectious (HIV) “high-risk core group” (Leber et al., 2008, p.404). Likewise, Zetola and Klausner (2007) suggest that the increased rates of syphilis among MSM are largely due to high risk sexual behaviour like serosorting (finding sex partners who are also HIV positive), safe-sex fatigue, and the success of anti-retro viral treatments that prolong or maintain a healthy sex life.
Syphilis is also said to increase the rate of HIV transmission “up to five times” (Pao et al., 2002, p.1448). Stated briefly, dormant asymptomatic syphilis when contracted with HIV, progresses rapidly to late syphilis. Symptoms like headaches, rashes, weakness in the limbs, and loss of hearing, sight and hair have led many to be tested and diagnosed with neuro, ocular and gummatous syphilis (Hay et al., 1990). Hence, it is evident that the protean manifestations of syphilis are far more detectable in a population of already immune suppressed individuals than they would be in the general population.
Are there underlying deleterious social circumstances that are capacitating this apparent syndemic interaction of syphilis and HIV among men who have sex with men? The question itself may be very straightforward when assessing data for a community of visible minorities, a geographic region, or neighborhoods that are linguistically, racially, or ethnically distinct, as have been shown by Farmer (1999) in Haiti, Singer (1996) and Singer et al (2006) for inner city Puerto Ricans and African-Americans in Hartford, Connecticut. However, MSM do not constitute such a measurable community. Though various case studies do indicate that there are instances of depression, isolation, and recreational drug use among some HIV positive males, and among syphilis HIV co-infected males, these vary, and are based on small random studies from various parts of North America and Europe (Reynolds et al., 1998; Operario and Nemoto, 2010; Stall et al., 2007; Gorbach et al., 2011; Wong et al., 2005).
Syndemic theory proposes that most infections and life threatening diseases interact with others and are concentrated in particular populations due to complex interactions between the environment and over riding socio-political conditions (Farmer, 1992; Singer et al., 2006). However, it is challenging to use a syndemics framework to assess the prevalence of syphilis among MSM who are HIV positive. Socio-economic and political factors such as poverty, violence, domestic abuse, unemployment, and racism are integral to syndemic theory but in this case they may, or may not apply. MSM is a large, faceless all encompassing term that defines everyone who is male and who has ever had sex with another male. Like the terms “culture” and “population” its boundaries are everywhere and yet nowhere.
An example of how amorphous relationships between disease and community are relentlessly imposed, can be observed in Singer’s (2010, p. 29) assertion that HIV was first observed among gay men, and then “it became a disease of the poor and ethnic minorities in the United States”. This statement certainly implies that gay men are not poor, nor part of any ethnic minority, and that HIV can move out of one community and into another with distinguishable and measurable boundaries in place. Furthermore, that particular socio-economic and political conditions that create and sustain the occurrence of the disease, can actually maintain these boundaries.
The reality is that men, whether they decide to have sex with other men long-term, occasionally, or never again, can be members of various communities, visible minorities, or majorities, especially in large urban centers. Conversely, gay men are not always part of a well-defined community because they represent a multitude of identities, races, and socio-economic backgrounds. Nonetheless, the boundaries of where one community, population or culture begins and ends are as challenging to define as the temporal and spatial limits of an epidemic. No community within any large urban centre exists as a remote and inaccessible entity, and no infectious disease is able to distinguish one community from another. Yet, the data on the occurrence of syphilis in the city of Toronto indicate that there have been very distinct spatial boundaries established as a result of a particular population’s interactions with a sexually infectious disease. Men who have sex with men are identified as a ‘community’ because a sexually infectious disease is apparently re-emerging among them.
In North America, the AIDs era clearly defined and demarcated a gay community with negative associations due to fears of contagion and stigma, but one of the major effects of the epidemic was the politicization of those diagnosed with AIDS (Gorman, 1986). The “gay community” – a group of socially active and politically engaged individuals– assumed control of the scourge, and fought for funding, access to health resources and social programs. Gorman (1986, p.167) asserts that “at no time in medical history has a group of afflicted people so rejected the role of being the sick and helpless victim”. The boundaries created around the population may have been ethically imposed with negative parameters, but they were ethically preserved in order to provide a culture-specific model of access and treatment. The first pamphlet on “Safe Sex” was written and distributed by a gay sex-trade worker in the S&M gay underground, and panel discussions between gay activists on television debated condom use while demanding access to medical treatment (Berkowitz, 2003).
An overview of various gay websites, and the AIDS Committee of Toronto website (ACT- see “Syphilis: It’s serious. And it’s here”.), as well as pamphlets in the Hassle-Free clinics across the city, indicates that the gay community is actively mobilizing, as they once did during the early days of AIDS, to disseminate information to the gay public on the current increase of syphilis.
Strategies for risk reduction, accessing health resources, screening and treatment specifically targeted to the “gay” and “queer” community in Toronto have been rapidly and efficiently implemented. Gay men for example are encouraged to take a survey on syphilis and to follow it up with a free syphilis test at any walk-in clinic (ACT, 2010). Public bathhouses in the city have also become sites where Hassle-Free staff offer free syphilis tests, along with condoms and lubricants (ACT, 2010). Men with HIV are urged to get their doctors to test them for syphilis since “physicians do not routinely test for syphilis anymore” (Toronto Public Health, 2010). Featured on many sites is a popular image designed in 2010, in the style of a sci-fi horror movie poster (see Figure 4). It advertises the return of syphilis as a green, razor-toothed monster wrapped around a young, semi-nude man. It is apparent from the website and public health material that an already highly organized and politicized group has quickly mobilized to define and control the limits of this new outbreak among them.
Whether the ads and the outreach programs are effective remains to be seen but the infrastructure of education, information, prevention, screening and treatment is firmly in place. Gay men, or any man who has sex with another man, have access to information, and can enter any walk-in clinic, get tested and treated for syphilis anonymously, and free of charge.
Figure 4. Poster for Syphilis Prevention from ACT (2010)
Within the mainstream population of Toronto, however, there does not seem to be a syphilis eradication or education program in place. The implicit message is that one is not needed due to the relationship and association that has been established between syphilis and an MSM community. Though information on syphilis is provided in all of the public health websites throughout Ontario, and statistics indicate that syphilis rates are increasing overall, the education, screening, and treatment platform stops there. No one else in the general population is being encouraged to get tested unless they ‘think’ they have syphilis, and if they do, they are advised to see their doctor.
Syphilis Cycles and Trends
The current trend of increasing rates of syphilis in Europe and North America is cast in the literature as evidence of a “worldwide” outbreak scenario. An old disease that was once well-known is returning with renewed vigour, and for reasons largely unknown. Based on a cursory review of some of the most recent articles, the “re-emergence” of syphilis is perceived as surprising and quite sudden.
By the year 1999 to 2000, a “sharp rise”, “outbreak” or “epidemic” is reported to be occurring primarily among MSM worldwide (Fenton et al., 2008; Klausner et al., 2005; Kofoed et al., 2006; Wong et al., 2005; Abraham et al., 2005; Kararizou et al., 2006; Montoya et al., 2005; and Chen et al., 2007). The reasons given for this sudden increase range from changing immunity and the biology of the disease, to issues around high-risk sexual behaviour, increased sexual networks, social media, HIV coinfection, and successful HIV drug therapies.
Researchers and scientists from a variety of disciplines and countries describe syphilis in historic terms, explain some of its stage-related manifestations, provide an update of its clinical features, and then proceed to document case studies that yielded surprising results. In all of the case studies, syphilis was not diagnosed until definitive tests were administered. For example, there were patients who presented with syphilitic skin rashes that were misdiagnosed as psoriasis (Dylewski and Duong, 2007); 10 individuals who were diagnosed with purulent tonsillitis who had oral syphilis (Xiushan, 2003); and last but certainly not least, there were 8 individuals with otosyphilis that were misdiagnosed with tinitis (Mishra et al., 2008).
From Greece to China, Russia to Denmark, France, Israel, the United Kingdom, Australia and North America this apparent phenomenon has been consistent. It would seem that the pattern of nondiagnosis–of syphilis, misdiagnosis–of other infectious ailments, and overdiagnosis due to comprehensive screening–of syphilis in the “MSM community” may be contributing to what appears to be a “sudden” epidemic among men alone.
In contrast to this Western trend, the figures in nonWestern countries are far more dire. According to the World Health Organization (WHO, 2007) there are 600,000 pregnant women who are newly infected each year with syphilis in Asia and the Pacific region. An estimated 2 million pregnant women in sub-Saharan Africa are infected, where 60 percent of these acute cases lead to fetal and infant death. Though the word “epidemic” or “outbreak” was never associated with the word syphilis in any of the WHO literature– it was a term reserved for HIV – an astounding 12 million new worldwide cases of syphilis occur annually, most of which go untreated (WHO, 2007). Thus, it would appear that the temporal and spatial limits of an epidemic are constantly being redefined depending on what and where disease occurs, and with what frequency. In Toronto, Canada for example, 500 cases a year of syphilis can determine an epidemic within a vaguely defined community, but 2 million cases a year of congenital syphilis among sub-Saharan African women constitutes an “ongoing public health concern” (WHO, 2008).
Clusters and Communities
Testing for syphilis in the province of Ontario used to be routine and part of a required screening program for immigration, obtaining a marriage license, pre-natal check-ups, and for healthcare workers. These were all discontinued by the late 1970s except for immigration requirements (Canada Immigration and HIV Reporting, 2010). Logically, the question then is whether syphilis is seen to be increasing among MSM and those who are coinfected with HIV, primarily because they are the only groups being tested. And if so, how does this data compare with another group that is routinely being tested, for example immigrants to Canada?
According to MacPherson and Gushulak (2008), elevated rates of syphilis were recorded in refugee claimants arriving in Canada, and between 2000–2004 the number of detected syphilis infections increased significantly by 90 percent. The ratio of male to female was 1:4. Males aged 56-65 years showed the highest rates at 324 cases (see Figure 5). For women aged 66 and older the rates were higher than the males of the 56-65 years of age category, and the 66 and older category (477 female cases compared with 439 male). A total of 56 children–14 and under–tested positive for infectious syphilis during this study period.
They note however, that there were inconsistencies in both reporting and testing due to the fact that late non-infectious cases are not nationally reportable, cases that are diagnosed and managed abroad are not necessarily reflected in the notifiable disease reports, and that there are often significant time delays between when a claimant is tested and the notification of public health authorities.
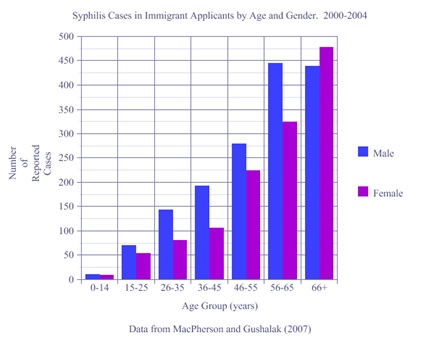
Figure 5. Syphilis Cases in Immigrant Applicants. Data from MacPherson and Gushulak (2007)
Moreover immigrants who travel back to “endemic regions of syphilis transmission” are not monitored or tested upon their return. As such, their findings “cannot be directly related to national syphilis reporting for the same time period” (MacPherson and Gushulak, 2008, p. 4). Their study is therefore a call for early diagnostic and consistent treatment services, specifically for refugee populations.
In 1998 Reynolds et al. reported an increase in rates of infectious syphilis in an immigrant population over a five-year period (1990–1994). One thousand residents in a suburb of Toronto (Scarborough) were newly identified in this study period as having positive syphilis serology (Reynolds et al., 1998, p.250). One in five cases was identified during immigration screening. In contrast to the infectious rates of syphilis in Ontario, they report that “syphilis was detected more often in younger adults yielding a male-female ratio of close to one” (1998, p.251).
When compared with the overall incidence of syphilis in the province however, they noted inconsistent rates that indicated a decrease. They attributed this to a decrease in detection due to lack of testing, and cited that there was a correlation of 0.95 between the provincial incidence of syphilis and the number of tests ordered. The data, as in MacPherson and Gushulak (2008), showed incidence rates of syphilis increased with successive age groups, the highest being in the 50-69 years of age category for both male and female (see Figure 6).
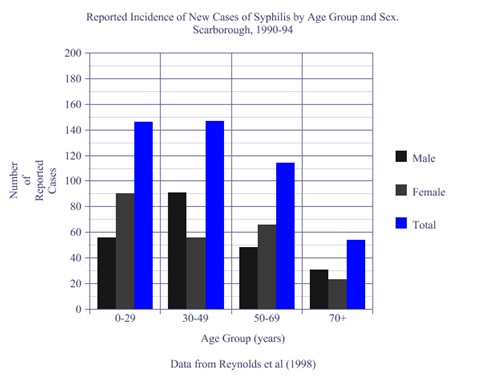
Figure 6. Reported Incidence of Syphilis in Immigration Screening. Data from Reynolds et al. (1998, p. 250)
Both Reynolds et al (1998) and MacPherson and Gushulak (2008) stressed the inherent difficulties in the public health management of syphilis in immigrant populations due to the problems of tracking highly mobile refugee claimants, definitive testing methods, and conducting follow-ups. Inconsistent reporting and the decreasing familiarity among healthcare workers with diagnosis and treatment added to the problem. They warn that the large proportion of untreated and treated syphilis “among foreign born as detected by immigration screening” requires better follow-up and management (Reynolds et al., 1998, p.252).
Combined with the complicated transmission and treatment issues of syphilis, a common complaint in several research articles, including Reynolds et al (1998) and MacPherson and Gushulak (2008), has been around effective and consistent testing (Kent and Romanelli, 2008; Pao et al., 2002; Leber et al., 2008; Mishra et al., 2011). Margulis et al. (2009) contend that there are no “reliable definitive tests for the presence of T. pallidum other than high magnification observation of the spirochetes or their round bodies in affected tissue by an experienced expert microscopist” (2009, p.54). Nevertheless, the accurate diagnosis of syphilis still “continues to elude and perplex many clinicians” (Mishra et al., 2011, p. 190).
When considering the current data from Toronto Public Health, the figures certainly reflect a rising infectious disease cluster among “MSM”. Supported by a variety of case studies, the Western trend seems alarming and worldwide. However, when examining the WHO’s figures (Figure 7) and the few studies that focus on immigrant and refugee populations, the Toronto Public Health Data, along with the North American and European data may in fact represent a testing cluster rather than an epidemic.
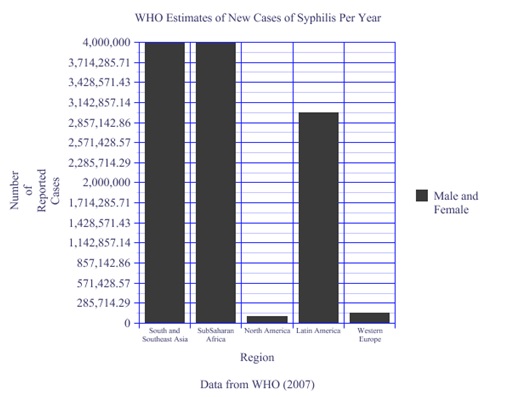
Figure 7. WHO Estimates of New Cases of Syphilis per year. Data from the WHO (2007)
Since syphilis is no longer routinely tested for, or even accurately diagnosed in the general population, it obviously cannot be reported. Public health bulletins insist that people get tested ‘if they think they might have syphilis’ and provide a list of symptoms that ‘they may or may not have’. In addition, current tests for syphilis like the VDRL (venereal disease research laboratory) and the RPR (reactive plasma reagin) can appear negative when patients have primary lesions, and even when they are in the latent stages of the disease (Birnbaum et al., 1999).
Nevertheless, when syphilis is tested for within various groups, as in immigrants, refugees, and gay men, it is found to be prevalent. This suggests that the epidemic’s temporal and spatial boundaries are far more culturally constructed than epidemiological. Unless these are the “core groups” engaging in “high-risk sexual behaviour, sero-sorting and safe-sex fatigue”, the consistently high rates of syphilis upon testing indicate other factors at play. In other words, the recent data may not be reflecting a new and vigorous outbreak that is part of a worldwide trend among MSM, but more analogous to what Fracastoro surmised 5 centuries ago; that as an “epidemic distemper” syphilis has been present so long in the population it is no longer recognized, or remembered by name (Fracastoro, 1930, p. 740).
Penicillin and Perpetual Grief
With the advent of penicillin-antibiotics, syphilis was considered a curable and thus eradicable disease. However, in a dramatic departure from mainstream medicine, Margulis (2004) and Margulis et al. (2009) maintain that syphilis “still prevails” and is not cured by antibiotic treatments but rather “driven underground”. They argue that it has not been adequately shown that “T. pallidum infection in its secondary and later stages is curable after any therapy” (Margulis et al., 2009, p.55). Their research on the evolution of spirochetes demonstrates that both Treponema pallidum (syphilis) and Boerrelia burgdorferi (Lyme disease) which are active, motile helical swimmers, revert to what are called “round bodies” when they are threatened by changes to their environment. Such changes include the presence of antibiotics, and other assaults like temperature changes, desiccation or starvation (Margulis et al., 2009, p.52). Apparently, spirochetes are not killed off after exposure to antibiotics, but are still viable and reproductive though they may be slower and less mobile. When conditions become more favourable, they revert back to their previous and more active morphology.
Margulis et al. (2009) reiterate throughout their report that antibiotics such as penicillin “and its derivatives” induce round body formation, and a suppression of symptoms rather than a cure. Though current medical opinion does not recognize the clinical significance, or relevance of round bodies (Margulis et al., 2009), many studies cited or reported deleterious side effects, failed treatments and relapses with the use of antibiotics for syphilis, especially in its later stages (Leber et al., 2008; Baughn and Musher, 2005; Bayne et al., 1986; Berry et al., 1987; Jorgensen et al., 1986). Baughn and Musher (2005, p.213) demonstrated that a staggering 79 percent of patients who were treated for secondary syphilis with penicillin developed increased prominence of lesions and high fever.
The question remains that if antibiotics do not cure syphilis, can it be said that the disease has been effectively controlled? McKenna (cited in Margulis, 2004, p. 122) stresses that spirochetes, namely T.pallidum, can exist in human tissue for decades and “their survival in any host, and despite any known therapy is nearly certain”. Margulis et al (2009, p.55) maintain that many people, both untreated and treated, carry the latent disease which has become invisible, referred to as the “syphilization effect”. But rather than lying dormant while round-bodied, spirochetes can still suppress the immune system. According to Radolf and Lukehart (2006) and Margulis et al. (2009), this may explain the high correlation between the presence of T. pallidum round bodies, and opportunistic infections, such as viruses and pneumonias.
The syndemic, or rather synergistic association between HIV and syphilis is therefore not a recent phenomenon, but may actually indicate a more historic and symbiotic relationship. In 1982 the first HIV isolate was identified from “Patient 1”, a 33 year-old Caucasian male (Barre-Sinoussi et al., 1983). He did not have AIDS but had been previously treated for syphilis, and Margulis et al (2009) doubt that he had been cured at all. They postulate that the narrow focus on HIV as the cause of AIDS “has facilitated missed diagnosis of syphilis” and its inherent relationship with autoimmune diseases (2009, p.55). Likewise, the assumption that penicillin-antibiotics have cured individuals of syphilis who then contract HIV rejects the integral role that syphilis has on the immune system, not to mention its ability to withstand a variety of drug treatments.
The history of AIDS thus appears to be intimately tied to the presence of syphilis. It has been shown that AIDS symptoms have always shown up with syphilis, and areas where there are high rates of AIDS include a high incidence of syphilis (Schmid, 2004; Margulis, 2004; Coulter, 2004). Most AIDS patients, according to Coulter (2002) show evidence of a past or present syphilis infection (see also Margulis, 2004; Smith and Canalis, 1998). Coulter (2002) ventures further by stating that the genesis of AIDS has largely been misunderstood by medical authorities who have dismissed syphilis in favour of HIV as a diagnosis for AIDS. He asserts that in the great majority of cases, AIDS is due to an already deteriorated immune system caused by syphilis, which then facilitates HIV transmission.
In light of this historic and synergistic association between AIDS/HIV and syphilis, the fact that there is a “worldwide epidemic” of HIV (WHO, 2008) not confined to the MSMs of Europe and North America, suggests that the status and attention should be accorded to syphilis given its primary role in HIV transmission and AIDS. However, Coulter (2002, p. 6) states that a viral theory of AIDS is unlikely to be superseded by a treponemal theory because of an already well-established “superstructure” that supports more prestigious research on HIV. Coulter adds that with a new disease such as AIDS, a new agent like HIV would enhance its mystery, power and authority, and syphilis is considered too old a disease to have a primary role in any medical advances.
Conclusion
The rise of syphilis among a specific cohort of men in Toronto, documented in graphs and charts, certainly demonstrates an outbreak. But when compared with other data, like the studies on immigrant and refugee populations, the same outbreak pattern is apparent. Considering the figures of venereal syphilis worldwide, it is possible that the local “outbreak” is more likely the visual representation of a testing cluster. The sudden ‘reappearance’ of syphilis is increasingly being noted among a group of men who are actively seeking, or being encouraged to get tested, primarily due to the rapid physical manifestations of the disease caused by co-infection with HIV. Among other groups from a variety of countries, who are legally required to be tested for entry into Canada, the disease is also prevalent, and is also seen to be increasing.
Unless a confluence of symptoms are presented, the disease goes unnoticed and untested in the general population. Yet even when classic symptoms of syphilis are apparent, as demonstrated in many of the case studies cited, it is often misdiagnosed due to unfamiliarity with the disease and its protean manifestations. Furthermore, syphilis is historically known for its ability to mimic other infections and consequently remain unrecognized and undetected.
The possibility that it has not been effectively eradicated with penicillin-antibiotics for the last 60 years raises even more questions regarding its present etiology, and the parameters of its transmission and occurrence. As a consequence, a small sample in the city of Toronto comes to reflect a much larger, worldwide scenario. This leads one to ask how a fatal infectious disease like syphilis moves from the status of invisible and endemic to visible and epidemic when geographic borders are crossed, and notions of a population are redefined. The inconsistent figures in distinguishing an “epidemic” from a “health concern”, as in 500 cases a year in Toronto versus 2,000,000 a year in sub-Saharan Africa, prove that it is not about the numbers of people afflicted, but more about who is infected and where.
Nonetheless, interest in syphilis has recently been revitalized due primarily to its persistent worldwide rates, and recognition of the fact that it is a major cofactor in the transmission of HIV (Radolf and Lukehart, 2006). Sir William Osler (1849–1919) stated at several points in his illustrious medical career that “syphilis is the only disease necessary to know” (Bean, 1950, p.134), and this is becoming more evident despite HIV’s current reign as the virus responsible for the world’s largest epidemic (WHO Global Summary, 2009).
With over 500 years of transforming culture, organizing modern medicine and informing Western civilization, the power attributed to this fatal infectious disease cannot be disputed. Indeed, a new generation of syphilologists marvel at its “stealth” ability to invade diverse organs, evade host defences, and maintain persistent infection in every part of the human body (Radolf and Desrosiers, 2009). Articles and books highlighting some of the more famous musicians, artists, writers and philosophers that suffered from syphilis are ‘re-emerging’ as part of a literary trend to place genius amidst treponemal madness once again (Golomb et al., 1999; Hayden, 2003; Margulis, 2004; Franzen, 2008).
Syphilis may have been eradicated from our collective memory, and replaced by a new venereal scourge, but rather than being relegated to the pages of forgotten history, it has been busy eluding science, medicine, public health, literature, history and the arts. As it distinguishes its own temporal and spatial boundaries, syphilis has seemingly continued its sovereignty as an “epidemic distemper” that many are only now beginning to remember by name.
Notes
- Over 1/3 of Paris was said to have been infected (Cartwright, 1972) and by the late 19th century approximately 10% of Europe was afflicted (Sherman, 2006).
- It was also known as the “Italian”, “Russian”, “French” or “Polish” scourge depending on political hostilities and fashion trends (see Sherman, 2006; Cartwright, 1972).
- As part of the United States Public Health Service Program funded by the National Institute of Heath, local prostitutes in Guatemala infected with syphilis were sent into prisons to have sex with male prisoners, or when that proved inadequate, the prisoners were inoculated with the pathogen (Bristol, 2010).
- Farmer (1999) as a medical anthropologist and physician working in Haiti, refers to this web of components as “structural violence” rather than syndemics.
- The acronym MSM was initially adopted to reduce the stigma of AIDS when it was considered primarily a “gay disease” (Dowsett, 1980).
References
Aadland, D., Finnoff, D., Huang and Kevin, X.D. (2007), “Syphilis cycles”, Munich Personal ReREc Archive, available at http://mpra.ub.uni-muenchen.de/8722/ (accessed 24 January 24 2011).
Abraham, B., Marih, L., Thevenet, T., Da Silva Marechal, E., Verdet, C., Rozenbaum, W. and Pialoux, G. (2005), “Outbreak of syphilis among HIV-infected patients: descriptive data from a Parisian hospital”, Sexually Transmitted Diseases, 32 (11), pp. 718-719.
ACT AIDS Committee of Toronto (2010), available at: www.actoronto.org/syphilis (accessed 13 March 2011).
Barré-Sinoussi, F., Chermann, J., Rey, F., Nugeyre, M., Chamaret, S., Gruest, J., Dauguet, C., Axler-Blin, C., Vézinet-Brun, F., Rouzioux, C., Rozenbaum, W., and Montagnier, L. (1983), “Isolation of a T-Lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS)”, Science New Series, Vol. 220 (4599), pp. 868-871.
Bates, A. (2008), “Indecent and demoralising representations”: public anatomy museums in mid-Victorian England”, Medical History, Vol. 52, pp. 1-22.
Baughn R., and Musher, D. (2005), “Secondary syphilitic lesions”, Clinical Microbiology Reviews, January, 18 (1), pp. 205-216.
Bayne, L., Schmidley, J. and Goodin, D. (1986), “Acute syphilitic meningitis. Its occurrence after clinical and serologic cure of secondary syphilis with penicillin”, G Arch Neuro, Vol. 43, pp.137-138.
Bean, W. (1950), Sir William Osler: aphorisms from his bedside teachings and writings. Collected by Robert Bennett Bean, M.D. (1874-1944)? Henry Schuman, New York.
Berkowitz, R. (2003), Stayin Alive: The Invention of Safe Sex, Westview Press.
Berry, C., Hooton, T., Collier, A. and Lukehart, S. (1987), “Neurologic relapse after benzathine penicillin therapy for secondary syphilis in a patient with HIV infection”, New Eng J Med, Vol. 6, pp.1587-1589.
Birnbaum, N., Goldschmidt, R. and Buffet, W. (1999), “Resolving the Common Clinical Dilemmas of Syphilis”, American Family Physician, available at: www.aafp.org /afp/990415ap/2233.html
Brandt, A. (1988), “AIDS in Historical Perspective: Four Lessons from the History of Sexually Transmitted Diseases”, American Journal of Public Health, April 78 (4), 367-371.
Bristol, N. (2010), “U.S. reviews human trial participant protections”, The Lancet, 376 (9757), pp. 1975-1976.
Canada Immigration and HIV Reporting (2010), available at: www.ehow.com/facts_6748875_canada-immigration-hiv-reporting-law.html
Canadian Institute of Health Research (2008), available at www.cihr-irsc.gc.ca/e/37839.html
Cartwright, F. (1972), Disease and History, Thomas Y. Crowell Co.
Chen, Z.Q., Zhang, G.C., Gong, X.D., Lin, C., Gao, X., Liang, G.J., Yue, X.L., Chen, X.S. and Cohen, M.S. (2007), “Syphilis in China: results of a national surveillance programme”, The Lancet, Vol. 369 (9556), pp.132-138.
Chesson, H., Heffelfinger, J., Voight, R. and Collins, D. (2005), “Estimates of primary and secondary syphilis rates in persons with HIV in the United States”, Sexually Transmitted Disease, 32 (5), pp. 265-269.
Clark, E.G. and Danbolt, N. (1955), “The Oslo Study of the natural history of untreated syphilis: An epidemiological investigation based on a restudy of the Boeck-Bruusgaard material, a review and appraisal”, Journal of Chronic Diseases, Vol 2 (3), pp. 311-344.
Coulter, H. (2002), AIDS and Syphilis: The Hidden Links, B Jain Publishers Ltd.
Dylweski, J. and Duong, M. (2007) “The rash of secondary syphilis”, Canadian Medical Association Journal, 176 (1), pp. 33-35.
Dowsett, G.W. (1980), “Reaching men who have sex with men in Australia-an overview of AIDS education, community intervention and community attachment strategies”, Aust J Soc Issues, 25, pp.186-198.
Fabricius, J. (1994), Syphilis in Shakespeare’s England, Jessica Kingsley Publishers, London.
Farmer, P. (1992), AIDS and Accusation: Geography of Blame, University of California Press.
Farmer, P. (1999), Infections and Inequalities: The Modern Plagues, University of California Press.
Fracastoro H. (1930), De contagione et contagiosis morbis et eorum curatione, libri iii., translated by Wright, W.C., G.P. Putnam’s Sons, New York, NY.
Franzen, C. (2008), “Syphilis in composers and musicians–Mozart, Beethoven,
Paganini, Schubert, Schumann, Smetana”, Eur J Clin Microbiol Infect Dis, 27, pp. 1151–1157.
Fenton, K., Breban, R., Vardavas, R., Okano, J., Martin, T., Aral, S. and Blower, S. (2008), “Infectious syphilis in high-income settings in the 21st century”, Lancet Infectious Disease, 8, pp. 244-53.
Gilman, S. (1995), Health and Illness: Images of Difference, Reaktion Books Ltd.
Golden M.R., Marra, C. and Holmes, K. (2003), “Update on Syphilis: Resurgence of an Old Problem”, JAMA, 290 (11), pp. 1510-4.
Golomb, J., Santaniello, W. and Lehrer, R. (1999), Nietzsche and Depth Psychology, State University of New York Press.
Gorman, M.E. (1986), “The AIDS epidemic in San Francisco: epidemiological and enthropological perspectives” in Anthropology and Epidemiology,
Janes, C., Stall, R. and Gifford S. (Ed.), D. Reidel Publishing Company, pp. 157-172.
Goudreau, S.M. (2010), “Accounting for epidemics: mathematical modeling and anthropology in Plagues and Epidemics: Infected Spaces Past and Present, Herring, A.D., and Swedlund A.C. (Ed.), Berg Publishing, pp. 213-230.
Greenspan, R. (2006), Medicine: Perspectives in History and Art, Ponteverde Press, Alexandria, Virginia.
Hay, P., Tam, F., Kitchen, V. (1990), “Gummatous lesions in men infected with human immunodeficiency virus and syphilis”, Genitourin Med, 66, pp.374-379.
Hayden, D. (2003), Pox: Genius, Madness, and the Mystery of Syphilis, Basic Books, New York.
Herring, A. and Swedlund, A. (2010), “Plagues and epidemics in anthropological perspective” in Plagues and Epidemics: Infected Spaces Past and Present, Herring, A.D. and Swedlund, A.C. (Ed.), Berg Publishing, pp. 213-230.
Holcomb, R.C. (1938), Who gave the world syphilis? The Haitian myth, Archives of Dermatology, 37(4), pp. 735-736.
Howles, J. (1943), A Synoposis of Clinical Syphilis, The C.V. Mosby Co, St. Louis, MO.
Inhorn, C. and Brown, P. (1990), The anthropology of infectious disease, Annual Review of Anthropology,19 (89), pp.1-17.
Jones, J. (1993), Bad Blood: The Tuskegee Syphilis Experiment, Free Press, New York.
Jorgensen, J., Tikjob G. and Weisman, K. (1986), “Neurosyphilis after treatment of latent syphilis with benzathine penicillin”, Genitourin Med, 62, pp. 129-131.
Kararizoui, E., Mitsonis, C., Dimopoulos, N., Gkiatas, K., Markou, I. and Kalfakis, N. (2006), “Psychosis or Simply a New Manifestation of Neurosyphilis?”, The Journal of International Medical Research, 34, pp. 335-337.
Karp, G., Schlaeffer, F., Jotkowitz, A. and Riesenberg, K. (2009), “Syphilis and HIV co-infection”, European Journal of Internal Medicine, 20 (1), pp. 9-13.
Kent, M. and Romanelli, F. (2008), “Reexamining syphilis: an update on epidemiology, clinical manifestations, and management”, The Annals of Pharmacotherapy, 42, pp. 226-236.
Klausner, J., Kent, C., Wong, W., McCright, J. and Katz, M. (2005), “The public health response to epidemic syphilis, San Francisco, 1999–2004”, Sexually Transmitted Diseases, October supplement 32 (10), pp. S11–S18.
Kofoed, K., Gerstoft, J., Mathiesen, L. and Benfield, T. (2006), “Syphilis and human immunodeficiency virus (HIV)-1 coinfection: influence on CD4 T-cell count, HIV-1 viral load, and treatment response”, Sexually Transmitted Diseases, 33 (3), pp. 143-148.
Leber, A., MacPherson, P. and Lee, C. (2008), “Epidemiology of infectious syphilis in Ottawa”, Canadian Journal of Public Health, 99 (5), pp. 401-405.
MacPherson, D. and Gushulak, B. (2008), “Syphilis in immigrants and the canadian immigration medical examination”, J Immigrant Minority Health, 10, pp. 1-6.
Margulis, L (2004), On Syphilis and Nietzsche’s Madness: spirochetes awake! Daedalus, American Academy of Arts and Sciences.
Margulis, L., Maniotis, A., MacAllister, J., Scythes, J., Brorson, O., Hall, J., Krumbein, W. and Chapman, M. (2009), “Spirochete round bodies Syphilis, Lyme disease and AIDS: Resurgence of the “great imitator”?”, Symbiosis, 47, pp. 51-58.
Miller, B. and Hicks, C. (2010), “Syphilis and HIV: the intersection of two epidemics”, Journal Watch HIV/AIDS Clinical Care, 3, available at: http://aids-clinical-care.jwatch.org/cgi/content/full/2010/903/1
Mishra, S., Walmsley, S.L., Loutfy, M., Kaul, R., Logue, K. and Gold, W. (2008), “Otosyphilis in HIV coinfected individuals: a case series from Toronto,
Canada”, AIDS Patient Care and STDs, 22 (3), pp. 213-219.
Montoya, J., Kent, C., Rotblatt, H., McCright, J., Kerndt, P. and Klausner, J. (2005), “Social marketing campaign significantly associated with increases in syphilis testing among gay and bisexual men in San Francisco”, Sexually Transmitted Diseases, 32 (7), pp. 395-399.
Moore, M. (1939), “Syphilis and public opinion (spirochaeta pallida, homo sapiens and Mrs. Grundy)”, Archives of Dermatology and Syphilology, 39(5), pp. 836-845.
Nnonuka, E. and Ezeoke, A. (2005), “Evaluation of syphilis in patients with HIV infection in Nigeria”, Tropical Medicine & International Health, 10 (1), pp. 58-64.
Operario, D. and Nemoto, T. (2010), “HIV in transgender communities: syndemic dynamics and a need for multicomponent interventions”, Journal of Acquired Immune Deficiencies Syndrome, 55, pp. S91-S93.
Pao, D., Beng, G. and Bingham, J.S. (2002), “Management issues in syphilis”, Drugs, 62 (10), pp.1447-1461.
Rabelais, F. (1653), Gargantua and Pantagruel in the works of Rabelais, 1894, translated by Doré, G., Moray Press, available at: http://www.gutenberg.org/files/1200/1200-h/p1.htm
Radolf, J. and Lukehart, S. (2006), “Pathogenic treponema: molecular and cellular biology”, Immunology of Syphilis, Caister Academic Press, Wymondham, Norfolk, pp. 285-313.
Radolf, J. and Desrosiers, D. (2009), “Treponema pallidum, the stealth pathogen changes, but how?”, Molecular Microbiology, 72(5), pp. 1081-1086.
Reynolds, D., Evangelista, F., Ward, M., Notenboom, R., Young, E. and D’Cunha, C. (1999), “Syphilis in an urban community”, Canadian Journal of Public Health, 89(4), pp.248-252.
Richardson, R. (2001), Death, Dissection and the Destitute, Phoenix Press.
Rosenberg, C. (1992), “What is an epidemic? AIDS in historical perspective” in Explaining epidemics and other studies in the history of medicine, Rosenberg, C.E. (Ed.), Cambridge University Press, Cambridge, pp. 278-292.
Rosenberg, C. (2003), “What is disease?”, Bulletin of the History of Medicine, 77(3), Johns Hopkins University Press, pp. 491-505.
Sappol, M. (2002), A Traffic of Dead Bodies: Anatomy and Embodied Social Identity in 19th Century America, Princeton University Press.
Saussy, H. (2010), Partner to the Poor: A Paul Farmer Reader, University of California Press.
Schmid, G. (2004), “Economic and programmatic aspects of congenital syphilis prevention”, Bulletin of the World Health Organization.
Sherman, I. (2006), The Power of Plagues, ASM Press, Washington, D.C.
Singer, M. (1996), “Dose of drugs, a touch of violence, a case of AIDS: conceptualizing the SAVA syndemic”, Free Inquiry in Creative Sociology, (24) 2, pp. 99-110.
Singer, M. (2010), “Ecosyndemics: global warming and 21st century plagues” in Herring, A.D. and Swedlund, A.C. (Ed.), Plagues and Epidemics: Infected Spaces Past and Present, Berg Publishing, pp. 21-37.
Singer, M. and Clair, S. (2003), “Syndemics and public health: reconceptualizing disease in bio-social context”, Medical Anthropology Quarterly, 17 (4), pp. 423-41.
Singer, M., Erickson, P., Badiane, L., Diaz, R., Ortiz, D., Abraham, T. and Nicolaysen, A. (2006), “Syndemics, sex and the city: Understanding sexually transmitted diseases in social and cultural context”, Social Science & Medicine, 63(8), pp.2010-2021.
Smith, M. and Canalis, R. (1998), “Otologic manifestations of AIDS: The otosyphilis connection”, The Laryngoscope, 99 (4), pp. 365-372.
Sontag, S. (1988), AIDS and Its Metaphors, Picador USA, Farrar, Straus and Giroux, New York.
Stall, R., Friedman, M.S. and Catania, J.A. (2007), “Interacting epidemics and gay men’s health: a theory of syndemic production among urban gay men” in Wolitski, R.J., Stall, R., Valdiserri, R.O. (Ed.), Unequal Opportunity: Health Disparities Affecting Gay and Bisexual Men in the United States, NY: Oxford University Press, New York, pp. 251–274.
Toronto Data Fact Sheet (2011), available at: www.toronto.ca/toronto_facts/diversity.htm
Toronto Public Health Sexual Health Information (2008), available at: www. toronto.ca/health/ sexual health/sh_stds_syphilis.htm
Toronto Public Health Bulletin on Sexually Transmitted and Bloodbourne Diseases (2008), available at: www.toronto.ca/…/statistics_and_reports/annual_reports/ pdf/2008/2008_sti_ annual_report.pdf
Wallace, R. (1988), “A synergism of plagues”, Environment Research, 47, pp. 1-33.
Wheater, P., Cook, P., Clark, P., Syed, Q. and Bellis, M. (2003), “Re-emerging syphilis: a detrended correspondence analysis of thebehaviour of HIV positive and negative gay men”, BMC Public Health, 3, p. 34.
Wong, W., Chaw, J., Kent, C. and Klausner, J. (2005), “Risk factors for early syphilis among gay and bisexual men seen in an STD clinic: San Francisco, 2002-2003”, Sexually Transmitted Diseases, 32 (7), pp. 458-463.
World Health Organization (2007), Health Impact Assessment, available at: www.who.int/std_diagnostics/publications/manuals/Syphilis_Eng_14May07.pdf
World Health Organization (2008), Regional Strategic Action Plan for the Prevention and Control of Sexually transmitted Infections 2008-2012, available at: www.wpro.who.int/sites/hsi/home.htm
World Health Organization (2009), Global Summary HIV/AIDS, available at: www.who.int/hiv/data/2009_global_summary.png
Xiushan, Y. (2003), “Pharyngeal clinical features of 8 cases of syphilis”, Otolaryngology – Head and Neck Surgery, 10 (1), pp. 23-25.
Young, R. and Meyer, I. (2006), “The trouble with “MSM” and “WSW”: erasure of the sexual-minority person in public health discourse”, American Journal of Public Health, 95(7), pp. 1144-1149.
Zetola, N. and Klausner, J. (2007), “Syphilis and HIV infection: an update”, Clinical Infectious Diseases, 44, pp. 1222-1228.